 Two days in as a newly minted RN, and I am struggling. Everything is new. I’ve never worked at this hospital before, I don’t know anybody and to make matters worse I’ve thrown myself into the deep end taking a job as a critical care nurse resident on an IMCU/PCU/Telemetry unit. Our patients are sick or they are ok but ready to crump and decompensate on us in a split second. I’m that new nurse doubling back to the med room multiple times for supplies each time I get to a patient’s room only to realize I’ve forgotten something I need for the third or fourth time. Luckily I have a preceptor who is kind and patient and supportive. She wants me to succeed.
My patient I’ve taken for the day is sick; in fact she is dying. My preceptor and I cared for her yesterday as well. She is not responsive and on high-flow oxygen. She is puffy, at first I think she is just obese. I’m too green as a nurse to recognize this as a sign of third-spacing of fluid, which is when the body can’t keep fluids inside the cells or in the blood vessels and that fluid seeps into all the tiny microscopic spaces between cells. I’m too new to tell just how close to death she is, but I am about to learn. I do know that she has a history of COPD and is septic from its complications. We told her at the end of my first shift on the unit yesterday that her family is coming to see her in the morning. I hope she heard. Her family has arrived and discusses options with the doctor. They have agreed to transition her to “comfort care”, which means we will no longer be attempting to treat her illnesses, but will rather shift the focus of care to helping her be comfortable in the dying process while making that transition to the other side in the most peaceful manner western medicine knows how. In the comfort care order set is western medicine’s death-and-dying gold standard: a continuous morphine drip, backed up with Ativan, a sedative medication to control restlessness, agitation, confusion and anxiety and a handful of other medications like liquid tears, medications to dry up respiratory secretions and anti-nausea medications. I’ve run off to get the supplies needed to set up the morphine drip. I’m not going to forget anything. The last thing this family needs right now is a bumbling nurse who barely knows where the bathroom is, much less one demonstrating incompetence while their loved one passes on. I work slowly and methodically to make sure I set up everything correctly and start the drip. My patient’s granddaughter mentions that she is studying to enter nursing school and works as a nurse assistant. She tells here family about the Cheyne-Stokes breathing pattern she has just noticed in her grandmother. This is an abnormal breathing pattern in which a person alternates between breathing progressively deeper, and sometimes faster, followed by a gradual decrease in breathing and a temporary stop in breath called apnea. It is often an impending sign of death and she has picked up on it before me. The granddaughter has the advantage though; she is able to focus solely on her grandmother, while my vision is narrow and being squeezed tighter by stress and anxiety from everything that is new tome in this exact moment, which happens to basically be everything going on in my life currently. I’m barely capable of priming my patient’s morphine drip and getting her vitals, much less being able to see the big picture of my patient and the even bigger picture which involves caring for her family’s needs. My nursing vision is small and I don’t have the defenses yet that are needed to push back on the forces constantly seeking to make that vision smaller. I step out of the room to update the patient’s chart with the cares I’ve just provided. Not even five minutes pass and the granddaughter comes to grab me. She is flustered and thinks her grandma has passed. I return to the room. I brutishly feel for a carotid pulse, which is absent. The granddaughter states that her grandma has stopped breathing. I’m not exactly sure what to do. They didn’t teach us this part in nursing school. I look back to see my preceptor watching over me from the door. She quietly prods me to use my stethoscope to listen for any heart or lung sounds. I sheepishly turn back to my preceptor and state that I don’t hear anything and I believe she has passed. I don’t yet have the confidence to look up into this family’s eyes and deliver to them poignant but expected news that their loved one has passed. I will unfairly beat myself up about this for the next foreseeable future. My preceptor steps in and offers consolation and comfort to the family. We step out to give them some time and space to grieve with the body. It won’t be until a month or two later, after I’ve placed a few more patients on comfort care, that I better understand and more importantly come to terms with my roll as a nurse in the death and dying process. For some patients, our unit is the last stop on a progressively rickety train of life all too commonly plagued by years of physiological neglect or decades of chronic systemic physical deterioration. Patients either get better here or they don’t. And when they don’t, some families are ok with that and are ready to let their loved ones go. Other families struggle to let go or at least are caught off guard by the emotional assault related to impending acute loss or weighty decisions like doubling down on invasive care leading to intubation, ventilation, and transfer to the ICU. I’ve quickly learned as a new nurse the stark truth that in these moments of crisis, I am the one these families turn to for guidance, direction and support. Whether I have 2 days, 10 weeks or a year on the job, I am somehow, an expected (and trusted) expert attempting to guide families through the turbulence and stress of events that are just barely something more than foreign to me. It’s a part of the job I knew I was signing up for but in no way could have ever understood the burden of until I walked through the gates of nursing on the IMCU. Nursing school prepared me for the NCLEX and gave me the bare bones knowledge required to begin to think critically about my patients, but it in no way could have prepared me for the weightiness of staring death in the face on a semi-regular basis. It didn’t prepare me for having to note the time of death of a patient and deliver that news to a family, as far as I knew that was the doctor’s job. In my pre-RN life, my experience with death was minimal. I’d attended a funeral here and there and watched my extended family grieve for a cousin taken from us suddenly and perhaps unexpectedly. All of my grandparents passed on, but I was miles from their bedside. I’d never seen anyone die. I’d never felt the salience of that moment when someone takes his or her last breath. After a while the family was ready to leave. I couldn’t find the words to say beyond telling them I was sorry for their loss. My preceptor offered that she was a great patient and a sweet lady, but I didn’t know those things. It was my second day and I barely knew this patient. But perhaps my preceptor didn’t either, maybe she just knew the right time to offer some thoughtful words and provide a hug. And compassionate touch. I reflected later what a cold, sterile experience death in the hospital can be; and worse, I worried that I’d somehow unwittingly contributed to that type of experience for this family. That first patient death was a right-of-passage for me. It took me a while to process what it all meant. What I took away was that I did the best that I could in that moment, and looking back like many things in life, hindsight is 20/20. That first experience is now my litmus for how I will approach future encounters with death. We start out as nurses with minimal confidence and tunnel vision, but it is a beautiful thing to see ourselves grow and be able to take on more stressful situations and see more clearly the needs of our patients and their family. While doing post-mortem care for my patient, I offered a silent prayer for her. I didn’t know her well or for very long, but it felt like the right thing to do. When we were ready to transport her to the morgue my manager decided to accompany me. She showed me our hospital’s ‘books of the dead’, which are two very large ledgers documenting the names of all those who’ve died at our hospital. It is a record stretching back more than 50 years. I added my name next to my patient’s name and added some of the details surrounding her death. We flipped back through the pages, remarking on the weight and power of this record. It was impossible not to feel a part of something so much larger than myself in that moment. Here in this basement room of our hospital I inked my name into a chain of events that started long before I was born and that will continue on long after my name is perhaps been added to another book of the dead somewhere else. In some ways, as nurses, we stand as gatekeepers of death. We hold the keys to the medications and interventions doctors order. In most cases if we used those tools to hasten death we would be called murderers. However under the special circumstances of comfort care, this action is encouraged and sanctioned. Its taken me transitioning several patients to comfort care for me to become comfortable with this roll of nursing, but it is still something I struggle with at times. In essence the medications we provide for comfort at the end-of-life can potentially hasten death. However guided by the principal of beneficence we as nurses act to minimize suffering, through charity, mercy and kindness. No one is immortal and we cannot ultimately push off the bounds of death. We can however make that experience more tolerable and calm for our patients and their families, which hopefully, ultimately outweighs any commitment to nonmaleficence we may feel. As a nurse with strong religious inclinations, this has been something I’ve had to work to come to terms with. Those decisions are particularly difficult in cases where a patient and family are refusing care and intervention in spite of a provider’s belief and perhaps a personal belief that something more can be done. Later when we got back up to the unit from the morgue, my manager told me that it would be important for me to find a way to process death in this line of work. She shared that her method was to keep a list of the patients she cared for that died, and when that list gets full she goes to the ocean and lets that list go in some form of cathartic release. I reflected back to the prayer I offered in the room that day for my patient and decided that would be something I would take forward to bring closure for myself and to give to each of my patients I cross paths with who ultimately pass away. Looking back, she was certainly right. Here I am seven months later still processing those events. These are real people, with real lives we care for and their imprints will be left on us from time to time, sometimes when we least expect it. While I didn’t start keeping my own list that day, I do remember that patient’s name. And perhaps when my list gets too large to keep track of in my head, I’ll jot those names down, hike them to a beautiful mountaintop and devise my own catharsis to let them finally go.
0 Comments
Born to act... or at least learning how: My response to a mid-flight emergency 30,000 feet up8/22/2018  In December 2017, a few weeks after graduation from nursing school, I found myself on a Christmas Eve flight to Florida to spend the holiday with my in-laws. Being a poor recently graduated, unemployed prospective nurse, we booked a red eye flight out of Denver. I’m not usually one for sleeping on planes, its just not something that has ever come easy to me, so I read my book for the first hour of the flight. I’d like to say I was drilling flashcards or reviewing material for the NCLEX, which may in fact be true, but I honestly can’t remember at this point.
We had lucked out and got seats in an exit row on a Spirit flight, which for anyone who has ever been packed into a Spirit seat, knows is a godsend, and luckily nobody was seated in the row with us. I was seated in the window seat and decided I would try to get some sleep so I would be somewhat functional to celebrate Christmas when we arrived. I closed my eyes and leaned my head against the side of the plane attempting to drift off in the most unnatural sleeping position possible. It couldn’t have been more than five or ten minutes after I closed my eyes before I heard someone a few rows back shouting for help. “Please someone help, he’s not conscious! I don’t know what’s wrong!” These are not the most ideal choice of words anyone wants to be hearing traveling 500 miles per hour, 30,000 feet up in the sky. I’m not sure if it was machismo from just graduating nursing school or what, but I knew that I had to answer this call for help. In hindsight it could have helped that a couple weeks prior to this flight at my pinning ceremony, as I was seated in the front row, I watched as a fellow nursing student crossed the stage to be pinned. Meanwhile an elderly relative of hers crouched to take pictures in the aisle, when suddenly he began to struggle to get up and nearly fell over from a crouched position onto the floor. I just watched (and so did 35 other graduates in my cohort) as this elderly man wobbled. In my head I debated whether this was serious enough that I should take action, and worse callously thought about whether I should interrupt the ceremony to help. Finally our favorite professor and key note speaker decided he had seen enough and leapt into action jumping down from the stage and coming to this elderly man’s aide. I remember believing in that moment that Dr. Parker had waited as long as he could to see if any of us recent grads would rise to the call and only jumped into action when us newly minted nurse graduates failed to do so. For the record the old guy was fine, perhaps his knees were bad, or he was a little bit light headed and dizzy trying to stand up too quickly, but the point was I had let myself and Dr. Parker down. Answering the call for help isn’t always an easy thing to do. One of the simplest things I’ve learned since my pinning is that we can make that decision a non-decision by choosing in advance to help. This rule of thumb holds true coming to the aide of those outside of our job, as well as being quick to act when things start to go south or just don’t feel right about a patient when on duty at work. Then when the moment of truth comes we just have to act, we don’t need to deliberate about whether it is the right thing to do, we just need to get proximal to the event and do what we can to help. Back at 30,000 feet on Christmas Eve, I decided to act. I jumped out of my seat and moved a few rows back to find a couple seated in both of the aisle seats. The wife is on my left as I stand facing the back of the plane, and she is rightly hysterical about her husband seated to my right on the other side of the aisle. He is unresponsive with his head slumped onto his chest. I look up and down the plane and realize that no one else is coming to help, this is it, and it’s all on me. I, the recent nursing school graduate, have the most medical experience on this entire flight. What are the odds? No pressure right? The first thing I do is check my “patient” for a carotid pulse, which is absent or so weak I can’t palpate it. Now I’m thinking this guy is having a cardiac arrest, I’m literally going to have to do compressions on this flight. I release the man’s seat belt and try to arouse him by calling at him and asking if he is ok while squeezing his triceps. Now I am telling the passengers in the area that I need help moving this man to the exit row area where there is more room for me to work on this guy and we can start CPR. Nobody is moving; everyone is just looking at me, dear-in-the-headlights. “Seriously people, this is a freakin’ emergency!” I scream inside my head. Finally a woman seated directly behind my “patient” gets up to help me move him. As we start to grab him to move him out of his seat, the man’s eyelids open but his eyes are rolled back in his head. He begins to come to a little bit. As he becomes a bit more arousable I ask him if he is having chest pain or shortness of breath, which he denies. He states he has a headache and doesn’t feel right. He is lethargic and not all together with it. I decide to evaluate for a stroke, because it seems like a reasonable thing to do. So I have him smile for me, and raise his arms out in front of him. His speech is a little bit slurred and he is obviously confused about what is happening, but I don’t think he has had a stroke. At this point a flight attendant hands me a blood pressure cuff and a disposable stethoscope. I think I’ve been handling things pretty well up until this point, but I have a moment of panic with the blood pressure cuff and stethoscope in my hands. I absolutely hate using the disposable stethoscopes because you can’t hear anything. They are worthless, and I panic that I am not going to be able to get a reading on this guy’s pressure due to the subpar equipment. I decide that maybe he is dehydrated and simply passed out. This too seams reasonable. I recall a patient from my nursing practicum a month or two prior who had a similar look with his eyes rolled back in his head and no palpable pulse who collapsed in his chair when standing and pulling his pants up to be discharged. A vasovagal episode as we call it in healthcare which ultimately leads to fainting aka syncope. Maybe my current “patient’s” blood has been pooling in his legs from sitting so long during the flight and he is not getting good perfusion to his brain. I make a mistake, disengage, and drop the cuff and stethoscope to the floor and head down the aisle towards the galley to ask a flight attendant for some water or ginger ale. Looking back I think I fully intended to come back and check the “patient’s” pressure. I just was trying to buy myself some time and delaying the inevitable because I had already assumed I was going to fail. I also wish in retrospect I would have asked for the gentleman’s name so I could have called for him with his name to arouse him instead of shaking, squeezing him, and basically yelling at him to wake up. When I come back up the aisle there is another women there who has picked up the stethoscope and BP cuff and is taking my patient’s” blood pressure. She is a nurse. She has lots of experience. She is an angel. I breathe a sigh of relief that I don’t have to manage this crisis anymore on my own, but I am also upset with myself that I shirked getting this man’s vitals and this nurse has, unbeknownst to her, had to step in for me. I will learn a lot from this nurse it turns out. She asks the wife for the husband’s name, and introduces herself to the patient. Brilliant! And such common sense! A few minutes later, he starts to get sick, and begins to vomit on his pants and on the cabin floor. The lady who was going to help me move him from his seat to the exit row uses a barf bag to catch what’s left. It turns out she is also a nurse. The older experienced angel nurse is in charge now. She is getting a history of events leading up to the flight from the wife. Brilliant! He’s taken Ambien before the flight; they ate dinner at a restaurant in the airport. They shared their food; the wife is not feeling sick at all. I don’t recall his vitals specifically at this point unfortunately; I think he may have been a bit febrile and perhaps tachycardic and a bit hypotensive. I am helping to get a new cycle of vitals. I assess his pulse rate. The older angel nurse comments on my apple watch display. She says I’m smart to have the second hand displayed on mine; she doesn’t have that on hers. This makes me feel good. Our patient continues to vomit or dry-heave sporadically. Another flight attendant asks us if we’d like some oxygen for our “patient”. It can’t hurt. He brings us a cylinder and mask. From somewhere a medical kit has showed up. It has emergency medicines and other supplies in it. I get the idea to test his blood sugar. He doesn’t have a history of diabetes, but I think it could be useful to rule out. My wife is a type-I diabetic I return to my row and get her glucometer and a new lancet. He surprisingly does have a high blood sugar, not grossly high, but high, perhaps undiagnosed type II or a stress response. His level of consciousness sporadically wanes and rebounds when we arouse him. He is lethargic, a likely effect of the Ambien, but possibly a sign of something else going on. The experienced nurse gets permission from ground control via the pilot to start an IV and administer a 500mL bolus of normal saline. It turns out even at 30,000 feet, under extreme circumstances we need permission from the powers-that-be to take any invasive action. Our goal is to get the fluid in him before we land in Florida. We let the flight staff know they don’t need to reroute the flight. They’ve been busy reshuffling passengers in close proximity to other seats on the plane, giving us more room to work, and freeing others from the trapped stench of emesis in the area. I am doing a good job reassuring the wife and educating her on what we have been doing and what we think might be going on. The experienced nurse nails the IV on the first try. I’m relieved she is here. I have no confidence in my ability to stick a needle in someone yet, much less in the middle of a semi-crisis, 6 miles up in the sky. She asks me to prime the IV tubing. “I can do that,” I say with a smile. There’s not much more we can do. We keep an eye on our “patient” and reassure the wife the rest of the flight. The bolus of normal saline fluid administered through the IV finishes as we taxi to the gate. Everyone is asked to remain seated so that medical staff from the airport can board the plane. They bring a specialized wheelchair just wide enough to squeeze down the aisle. We give report to the medical staff, who busily jot down their notes. They ask the wife a few questions and whisk our patient and his wife off the plane. Our in-flight medical team, returns to our seats. We collect our families and our bags. The rest of the passengers give us a round of applause as we head up the aisle to deboard the plane. Our little medical team and our families have short debrief after we get off the jet way and into the terminal to process our surreal Christmas Eve flight. Passengers departing the flight stream by our little group, telling us thank you and offering other encouraging words as they pass by. We separate from each other with hugs, no longer the strangers we began the flight as, but as a team bonded by our shared experience. I still don’t know much about nursing, but I now know a little bit more about functioning as a team during a crisis, and the underlying bond those of us in this profession share. I spend the next several days, maybe weeks, mulling over what I did well, and what I could have done better. I’m probably too hard on myself; after all I am not even a real nurse. Yet. I don’t need to handle emergencies and crises perfectly. Yet (or ever). I just need to pass the NCLEX, that’s my next goal in sight. Besides there’s always room to be better in nursing, there’s always room to grow and more to learn. Thankfully, there is no substitute for experience either, and this one has pushed me closer towards my goal of being a proficient critical care nurse, in spite of any ineptitude I have. Interestingly I will spot our “patient” and his wife in the ticketing line as we check in for our return flight home from Florida to Denver. I don’t know if they see me, but I also don’t make any effort to be seen or to ask them what the outcome was. For some reason it doesn’t feel appropriate to call out the events of our previous flight or inquire about his health in the sea of all these new strangers. I also run into my new friend the experienced angel nurse, the anchor of our team. She too is returning to Denver on the same flight my wife and I will be on. We catch up about our time in Florida and our return to Colorado. We both remark that it’s funny that we are all here together again, our patient and the two of us. She mentions that she said hi to them. I don’t push her for details, for some reason I prefer not to know. The concourse and ticketing counters are packed. From down the open room someone calls out for help. “Is there a doctor here? Please someone help!” The nurse and I look at each other and shake our heads. “Unbelievable. You’ve got to be kidding me”, I say. She laughs and replies, “Seriously again?” We share a quick chuckle; I turn to begin weaving through the crowded hall toward my next patient in need and just a little bit more prepared. “Born to act”, I tell myself, “or at least learning how.” 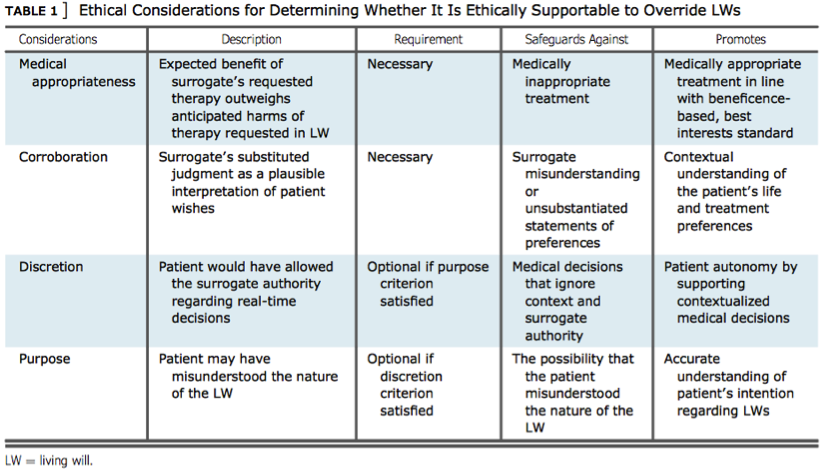 A patient’s right to autonomy and self-determination ideally should be absolute. The value of patient preference and choice regarding the care they receive is so high that the concept of advance directives (ADs) was created to act as a bridge of communication between incapacitated persons and the providers tasked with supporting a patient through some of their darkest days. While it can be easy to conceptualize ADs as bulletproof documents valiantly defending a patient’s right to autonomy and self-determination, the reality is that ADs can be overridden or (perhaps more shockingly) outright ignored in favor of provider preferences and surrogate family members interests. Perhaps it is simplistic to hold the ethical principles of autonomy and self-determination in such infallible and high regard, but it is astounding to learn that patient preference can and is often deferred at best in favor of a provider’s intrinsic responsibility to concepts of beneficence and nonmaleficence, and at worst in avoidance of drawn out legal battles or prioritization of surrogate family members interests. In all fairness to providers, ADs are complicated documents often executed in the middle of complex medical crises. It is impossible for an AD to be applicable to every single health crisis a person may encounter; and furthermore, a patient’s needs, interests and wants may change right in the thick of a hospitalization. Providers may simply not have time in the middle of a crisis to accurately interpret the wishes in an AD or the AD may not be clear or specific enough to be effective in a given crisis. More insidiously providers are trained to treat, heal, and fix patients at nearly any cost, and may have a difficult time executing an AD in favor of leveraging treatment they strongly believe will save the patient. Abadir, Finucane, and McNabney (2011) highlights this angst felt by one provider: “[This case] falls into a gray zone, where, while the DNR/DNI orders remain respected, we are faced with a possibly reversible clinical condition… At that point, it is difficult to stand there and let the patient slip away, knowing that perhaps it is just a pneumonia that could be cured with antibiotics and a couple days of life support. After all, this is why I am here, to help save lives and make people feel better.” For nurses prioritizing ethical principles of patient autonomy and self-determination, this statement should sound numerous alarm bells. Coded in this idea is that if the patient just could understand and see their health crisis from the provider’s perspective they would not hesitate to proceed with invasive and unwanted treatments specified in an AD. Provider relationships with family members can also interfere with a patient’s AD. Providers may believe they are doing the least harm to the family and promoting the greater good for the most people by choosing to honor surrogate family members’ wishes to extend life by overriding a patient’s AD. In doing so a provider chooses to prioritize utilitarianism and beneficence over patient autonomy, prioritizing closure for surrogates over a patient’s right to autonomy and self-determination through an AD. Surrogate family members beliefs and preferences also complicate implementation of ADs. Surrogates are all too often not included in discussions between patient and provider regarding an AD. This leaves family members out of the loop in understanding their loved one’s final wishes. Family members also often view ADs as abstract ideas relating to treatment and situations that are difficult to imagine. It can be hard for family members to conceptualize their loved one dying without any desire to continue fighting. The danger is when these conceptual situations become reality and family members have not been adequately prepared for the difficulties at hand, leaving some surrogates to prioritize their personal interests over their loved one’s claim to autonomy and self-determination. A quote from a doctor in Abadir et al. (2011) drives this point home: “If the patient comes alone, and no family can be reached, his or her DNR/DNI form will hold, but if a patient comes with family and is incapacitated, then the family makes the decision regardless of his DNR/DNI status, after the doctor has provided them with a rational and logical explanation.” It is clear from the above quotations that some providers have little to no inclination to validate an individual’s final wish in the face of challenging crises or challenging surrogate family members. The intrinsic complexities of ADs as well as provider and surrogate family member’s beliefs and preferences can leave a patient vulnerable to having their AD disregarded or overturned. Fortunately nurses are strategically positioned to advocate for patients both with providers and family members. Nurses can be well positioned to anticipate barriers to AD implementation by understanding the intricacies of ADs and the interests and beliefs of all parties involved. Nurses can leverage their face-to-face time with patients and families to determine the appropriateness of ADs on a case-by-case basis. Nurses can also be instrumental in aligning patient and family member’s interests and goals long before a health crisis even begins. Nurses must also be fluent with personal and organizational ethical frameworks in order to determine the validity of overriding an AD. “Absolute reliance on formally correct advance directives is not what many patients want”, with many patients desiring for loved ones and providers to have a say, “even if it contradicts a hypothetically ‘perfect’ living will” (Abadir et al., 2011). In sum many patients acknowledge they do not have all the answers during health crises and value input from those they trust. Nurses can only successfully balance the varying and complex priorities involved in ADs by understanding their own subjective ethical preferences and by leveraging ethical frameworks to decide which priorities are paramount. Bruce et al. (2016) outlines one such framework suggesting nurses consider the following factors when navigating ADs: medical appropriateness of interventions, corroboration with surrogates and family members, patient discretion and preference, and the patient’s intention of their AD. Ultimately by leveraging the above concepts, nurses are positioned to stand up to providers and surrogate family members as the need arises and advocate for execution of their patient’s AD. By using nursing judgment and investing time fostering relationships with providers, patients, and family members, nurses can see more clearly when ADs are being mismanaged, misunderstood or outright ignored. Patient safety and advocacy after all are primary concerns falling under the nursing scope of practice. While it certainly may be justifiable in some situations to stand up to providers, this is a late intervention. The preferable goal for nurses is to leverage valuable face-to-face time with patients and family members to promote education and communication while working to identify and overcome barriers to implementation of ADs. By doing so nurses are able to more fully promote patient autonomy and self-determination. Abadir, P. M., Finucane, T. E., & Mcnabney, M. K. (2011). When Doctors and Daughters Disagree: Twenty-Two Days and Two Blinks of an Eye. Journal of the American Geriatrics Society, 59(12), 2337-2340. doi:10.1111/j.1532-5415.2011.03700.x Bruce, C. R., Bibler, T., Childress, A. M., Stephens, A. L., Pena, A. M., & Allen, N. G. (2016). Navigating Ethical Conflicts Between Advance Directives and Surrogate Decision-Makers’ Interpretations of Patient Wishes. Chest,149(2), 562-567. doi:10.1378/chest.15-2209  I’m going to come right out and say it; maternal-newborn nursing is, in my opinion, hands down the most worthless class/rotation of nursing school. Obviously there are going to be some colleagues in my cohort and eventual practice who strongly disagree, but before you girls (and maybe guys) jump down my throat at the next lecture, hear me out. Perhaps a more polite way to sum up my position is this: OB is a giant elephant attempting to hide under NCLEXs bed. Think about it this way: According to U.S. Bureau of Labor Statistics (2008) there over 2.6 million practicing RNs in the United States. In contrast, according to the most recent National Sample Survey of Registered Nurses (NSSRN) conducted in 2008, only 5% of respondents identified Maternal-Child as their primary specialty, while an additional 2% identified Women’s Health as their primary specialty. Similarly, Illinois surveyed their RN workforce in 2015 and found 4% of respondents identifying Maternal-Child as their primary specialty and 2% of RNs identifying Women’s Health as their primary specialty. Admittedly it is problematic to extrapolate results from a national survey of RNs or one state’s findings as the status quo for the entire national nursing workforce. However the simple ugly truth of the matter is that the NCLEX considers questions regarding maternal newborn nursing fair game, and because we must pass the NCLEX to become an RN, we must study and know (at least temporarily) the ins and outs of our OB rotation. To consider this from the perspective of our investment in our nursing program, we are forced to spend roughly 8.5% of our time and money on a specialty that 4-5% of us will end up working in. It’s no secret that nursing school is just the first step towards a career as a nurse. There is too much to know and it is impossible to pick it all up in school. Hospitals know there is going to be a gap in knowledge and that they will have to onboard new grads and invest in them to bring them up to their full potential. In my opinion it doesn’t make much sense to spend 8.5% of our program focused and dedicated to learning information that is by and large going to go out the window for most nursing students within the first couple months or year after school, or even worse within weeks after the rotation. Nursing and healthcare are fields that pride themselves on being on the forefront and cutting edge. Medicine and nursing are constantly looking to innovate and move forward in the most positive direction, Furthermore we are learning how to become agents of that change through evidenced based practice by paying attention to not only the patient side of things, but the financial and institutional wellbeing of our future organizations. In my opinion, the OB rotation of nursing school is a glaring example of a lingering ugly appendage of nursing when it was a profession explicitly dominated by women wearing white shirts and skirts with a nursing cap sporting the red cross. It’s a relic from the days when the men were doctors who smoked on the unit and the women nurses were forced to give up their seats at the nurses’ station for those doctors to do their work. It curious to me that the profession has come so far and continues to evolve in so many positive ways yet has stayed so archaic on this particular front. How great would it be if this portion of the semester was spent allowing students to have focused independent or small group study in a specialty that interests them? The 2008 NSSRN reports the top five employed nursing specialties as follows: Other (20%), Acute/Critical Care (17%), Medical Surgical (13%), Geriatric (6%), and Pediatrics/Neonatal, Maternal-Child, and Home Health all tied for 5th (5%). Statistically speaking that time would be invaluable if there were say five tracks to cover the most in demand and common specialty tracks of nursing. Students would be more engaged with the material, hospitals would receive graduates who are better prepared for the positions they need, and hypothetically patients would have better outcomes by receiving an elevated standard of care from inexperienced nurses. Sadly the first major roadblock to any change like this has to be monetary. Such a change would require anywhere from 5-8 different versions of the NCLEX as one blanket version for all prospective RNs would be insufficient. Strain would also be put on educational institutions to create curriculum and provide adequate staffing for the various tracks. As it stands nursing students are likely stuck with the current academic model of the educational RN mill that preps students to pass the NCLEX as it is today, when the potential reality could be so much more. To be clear, I don’t hate my OB rotation. I am actually excited that we get to spend a day in the NICU, which ironically (and more appropriately) would fall under the potential Pediatrics/Neonatal track. I will also be prepared to attempt to deliver babies or at least care for mom and baby when the apocalypse strikes or at the very least if a precipitous birth and I ever cross paths. All joking aside I respect all nursing specialties and know that each type of nursing provides a valuable service. And honestly I'm a bit jealous of my classmates whose jam might be Maternal-Child health. They get to spend half a semester focused on what they want to really do, while I on the other hand contemplated buying a critical/intensive care nursing textbook off of Amazon, only to decide I was too busy learning OB and PEDs this semester to have that sort of distraction on my radar. Everything in good time I guess right? It would be silly to waste half of a semester not engaging in the material and the silver lining I’ve been able to find is that if I can learn and dedicate myself to OB, there is absolutely no reason I can’t learn the ins and outs of trauma and critical care nursing when the time comes. It’s one step at a time on the journey and right now that step involves learning everything there is to know about moms, babies, and birth, and vaginas. Please take the survey below or leave a comment. I’d love to hear if you feel OB has a place in BSN curriculum or if its outdated. Keep chasing your dreams and enjoy the ride. Happy studying to everyone out there. ‘Sadistic’ may be the most appropriate term to describe what it’s like to look back on the many many hours, days… even years invested in pursuit of a dream, while at the same time trying to wrap your head around the immense chasm of understanding, knowledge, and experience needed yet still. Nursing school and long term goals definitely fall under this umbrella.
At this point in my nursing journey I am metaphorically out of the harbor and out to sea. I am too far away from the shore to turn around even if I wanted to, but I also have no idea when the next time I will see land will be. I catch occasional little mirages of land, oases found in clinical rotations and class, which in real life equate to ideas, thoughts and action aligning. But all too often those moments are fleeting. In the next instant we’ve moved on to the next wave of material in class, or I don’t have a good answer or idea to why something is happening with a patient or case study, or I am botching some simple part of a procedure for the seventh time like setting down and contaminating a 10 mL flush to be split over the SAS on an IV push. Maybe that’s why they teach us to use two flushes in nursing school. (See that was a little oasis a ha moment right there just writing this.) *Non-healthcare provider readers, sorry to get technical there, if you’d like to understand what I’m talking about, check out the italic paragraph at the end for an explanation. That all might be a little dramatic, but at the very least, it’s a strange feeling to be caught somewhere in between still feeling so so far away from realizing a dream, and simultaneously reflecting on just how far you’ve come since taking the first steps towards a lofty goal. Today as I sat in this helicopter I couldn’t help but think about how far away from simply becoming an RN I sometimes feel, which makes complete sense because becoming an RN is not simple or easy. Over the last 5 months, as I have charted a course into the deeper waters of nursing, I’ve gained a better understanding of the complexities, challenges, and sheer cache of knowledge needed to excel as an RN, and it is overwhelming at times. The idea that I could literally save lives and have the knowledge to make split second life or death decisions on behalf of another person as an ICU and flight nurse someday is so weighty it seems almost unreal. It is a lot to take in knowing that landing back on dry land as an RN could merely be an island stopover on the way to solid footing as a critical care nurse. This idea could be teased out even further by visualizing flight nursing as merely just another island on the perilous "knowledge" sea crossing to becoming a nurse anesthetist. From where I stand now the scale and magnitude of these goals are bigger than I ever imagined. This is not to say or imply that lofty goals beyond the RN aren’t worthwhile or unattainable. They’re simply just very hard to conceptualize or be concerned about in relationship to the challenge at hand, which is learning and preparing for the NCLEX to earn RN after my name. The only answer I’ve come up with to overcoming seemingly insurmountable grandiose plans and ambitions has to be keeping the big picture or perspective simmering on the back burner while turning the heat up on the critical mix of ingredients up front. For a while in my nursing program I had left the steering and command of my ship of learning in the hands of more seasoned nurses and educators in both the clinical and classroom experience, which is completely understandable given my general lack of experience in this field. However over the last couple weeks of clinical rotations, I’ve had an epiphany that at this stage in the journey I actually do have some good ideas about how to care for people, and I have enough knowledge to make (or humbly offer up) suggestions regarding patient care with nurses I work and learn with. I can ‘turn the heat up’ and accelerate my learning by taking the rudder and steering my own learning when possible. Ways I’ve realized to accomplish this include spending more time considering the patient’s needs, spending more time personally educating patients regarding therapies and drugs, and even better, coming up with and sharing my own ideas about plan of care for a patient, including drug and therapy suggestions, questions, and concerns with the nurse I am working with. Unfortunately it is far too easy to settle into a passive clinical experience as a wallflower tethered to a more experienced nurse. It’s too easy to fall into the trap that they have more experience and defer to just watching them work and trying to learn by osmosis, or remaining closed mouthed and silent with thoughts and ideas because “they know better than us”. I’m sure everyone in my cohort has seen a nurse they are working with do something inappropriate or not by the book at this point. Do they really know better (or at least practice better) than us all the time? The answer is clearly no. Nursing is a contact sport, and when we choose passiveness, we ultimately are shying away from an optimized, active and engaged learning experience. We can watch other nurses operate, plan, assess and push meds all day, but until we actually attempt to initiate ideas and plans of care we are selling ourselves short by missing out on opportunities to critically think through care we are providing. Another strategy I have come to love this semester is asking ‘Why?’ about everything. Why does a particular pathology manifest with xyz signs and symptoms? Why is the patient on this drug? Why are these side effects associated with this drug or treatment? Why are we providing a particular course of treatment? Why? Why? Why? Asking these questions force us to think critically and make big picture connections instead of relying on and memorizing a million one-off facts. Putting these habits into play can be hard, but trying to regularly will allow us to develop routine that turns the heat up on current tasks at hand and promotes the ability to work more effectively, critically and confidently. The goal for us is to see the little steps we are taking moving us closer to our ultimate ambitions, whatever they may be. When we can note these small island mirages and oases we gain confidence in our skills and abilities and move a positive cycle forward. We can then occasionally find ways to ‘sample’ our simmering long-term plan to make sure that goal is still appealing and applicable. This might involve networking and talking with professionals in a career or specialty you are interested in or capitalizing on opportunities to experience other units or jobs and understand how each position requires different personality and focus. Success in nursing school, like many things in life, is enhanced by the effort put into it (Surprise!), and is navigated best through active engagement in the learning process. When we are staring down huge goals, its imperative to break them down into digestible chunks. And while it may feel impossible now that I could one day function productively on a flight-for-life crew or stand at the head of an operating table as a nurse anesthetist, I can be proud that today I learned to hold on to my 10 mL flush during an IV push and got more involved in managing my patient’s care. As they say it’s often the little things in life. *Non-healthcare provider readers: Sorry to get technical back there for a second. To bring you up to speed, when we nurses push a quick dose of medication through your IV, the process involves flushing the line with a saline flush before and after attaching the syringe with medication and administering it. This makes sure the line is patent and functioning properly before administration and makes sure all of the medication makes it in to your body and doesn’t just sit in the line after administration. We could use one larger flush to split between the two, but if the tip of our flush touches anything in the room in between the flushes it is considered contaminated, and I have a bad habit of disconnecting the flush and setting it down, which is a no no. The other option would be to use two smaller flushes and not even have to worry about this issue. |

Alexander McNaChronicles of my journey into the nursing profession. Archives
September 2018
Categories |
 RSS Feed
RSS Feed
