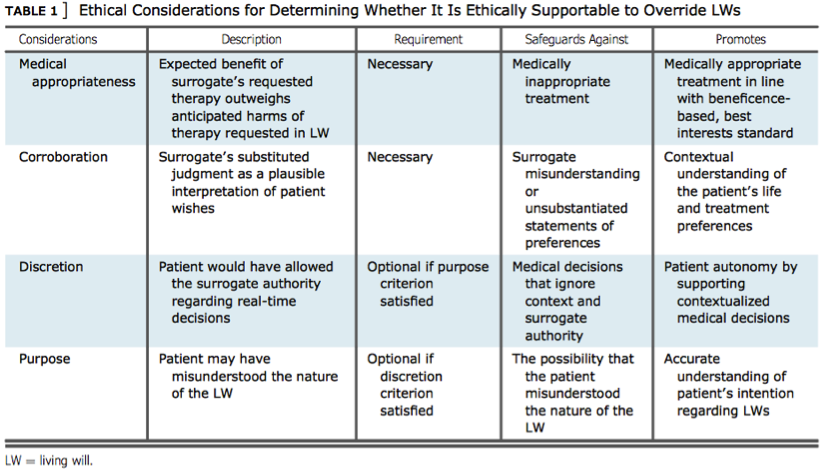
 A patient’s right to autonomy and self-determination ideally should be absolute. The value of patient preference and choice regarding the care they receive is so high that the concept of advance directives (ADs) was created to act as a bridge of communication between incapacitated persons and the providers tasked with supporting a patient through some of their darkest days. While it can be easy to conceptualize ADs as bulletproof documents valiantly defending a patient’s right to autonomy and self-determination, the reality is that ADs can be overridden or (perhaps more shockingly) outright ignored in favor of provider preferences and surrogate family members interests. Perhaps it is simplistic to hold the ethical principles of autonomy and self-determination in such infallible and high regard, but it is astounding to learn that patient preference can and is often deferred at best in favor of a provider’s intrinsic responsibility to concepts of beneficence and nonmaleficence, and at worst in avoidance of drawn out legal battles or prioritization of surrogate family members interests. In all fairness to providers, ADs are complicated documents often executed in the middle of complex medical crises. It is impossible for an AD to be applicable to every single health crisis a person may encounter; and furthermore, a patient’s needs, interests and wants may change right in the thick of a hospitalization. Providers may simply not have time in the middle of a crisis to accurately interpret the wishes in an AD or the AD may not be clear or specific enough to be effective in a given crisis. More insidiously providers are trained to treat, heal, and fix patients at nearly any cost, and may have a difficult time executing an AD in favor of leveraging treatment they strongly believe will save the patient. Abadir, Finucane, and McNabney (2011) highlights this angst felt by one provider: “[This case] falls into a gray zone, where, while the DNR/DNI orders remain respected, we are faced with a possibly reversible clinical condition… At that point, it is difficult to stand there and let the patient slip away, knowing that perhaps it is just a pneumonia that could be cured with antibiotics and a couple days of life support. After all, this is why I am here, to help save lives and make people feel better.” For nurses prioritizing ethical principles of patient autonomy and self-determination, this statement should sound numerous alarm bells. Coded in this idea is that if the patient just could understand and see their health crisis from the provider’s perspective they would not hesitate to proceed with invasive and unwanted treatments specified in an AD. Provider relationships with family members can also interfere with a patient’s AD. Providers may believe they are doing the least harm to the family and promoting the greater good for the most people by choosing to honor surrogate family members’ wishes to extend life by overriding a patient’s AD. In doing so a provider chooses to prioritize utilitarianism and beneficence over patient autonomy, prioritizing closure for surrogates over a patient’s right to autonomy and self-determination through an AD. Surrogate family members beliefs and preferences also complicate implementation of ADs. Surrogates are all too often not included in discussions between patient and provider regarding an AD. This leaves family members out of the loop in understanding their loved one’s final wishes. Family members also often view ADs as abstract ideas relating to treatment and situations that are difficult to imagine. It can be hard for family members to conceptualize their loved one dying without any desire to continue fighting. The danger is when these conceptual situations become reality and family members have not been adequately prepared for the difficulties at hand, leaving some surrogates to prioritize their personal interests over their loved one’s claim to autonomy and self-determination. A quote from a doctor in Abadir et al. (2011) drives this point home: “If the patient comes alone, and no family can be reached, his or her DNR/DNI form will hold, but if a patient comes with family and is incapacitated, then the family makes the decision regardless of his DNR/DNI status, after the doctor has provided them with a rational and logical explanation.” It is clear from the above quotations that some providers have little to no inclination to validate an individual’s final wish in the face of challenging crises or challenging surrogate family members. The intrinsic complexities of ADs as well as provider and surrogate family member’s beliefs and preferences can leave a patient vulnerable to having their AD disregarded or overturned. Fortunately nurses are strategically positioned to advocate for patients both with providers and family members. Nurses can be well positioned to anticipate barriers to AD implementation by understanding the intricacies of ADs and the interests and beliefs of all parties involved. Nurses can leverage their face-to-face time with patients and families to determine the appropriateness of ADs on a case-by-case basis. Nurses can also be instrumental in aligning patient and family member’s interests and goals long before a health crisis even begins. Nurses must also be fluent with personal and organizational ethical frameworks in order to determine the validity of overriding an AD. “Absolute reliance on formally correct advance directives is not what many patients want”, with many patients desiring for loved ones and providers to have a say, “even if it contradicts a hypothetically ‘perfect’ living will” (Abadir et al., 2011). In sum many patients acknowledge they do not have all the answers during health crises and value input from those they trust. Nurses can only successfully balance the varying and complex priorities involved in ADs by understanding their own subjective ethical preferences and by leveraging ethical frameworks to decide which priorities are paramount. Bruce et al. (2016) outlines one such framework suggesting nurses consider the following factors when navigating ADs: medical appropriateness of interventions, corroboration with surrogates and family members, patient discretion and preference, and the patient’s intention of their AD. Ultimately by leveraging the above concepts, nurses are positioned to stand up to providers and surrogate family members as the need arises and advocate for execution of their patient’s AD. By using nursing judgment and investing time fostering relationships with providers, patients, and family members, nurses can see more clearly when ADs are being mismanaged, misunderstood or outright ignored. Patient safety and advocacy after all are primary concerns falling under the nursing scope of practice. While it certainly may be justifiable in some situations to stand up to providers, this is a late intervention. The preferable goal for nurses is to leverage valuable face-to-face time with patients and family members to promote education and communication while working to identify and overcome barriers to implementation of ADs. By doing so nurses are able to more fully promote patient autonomy and self-determination. Abadir, P. M., Finucane, T. E., & Mcnabney, M. K. (2011). When Doctors and Daughters Disagree: Twenty-Two Days and Two Blinks of an Eye. Journal of the American Geriatrics Society, 59(12), 2337-2340. doi:10.1111/j.1532-5415.2011.03700.x Bruce, C. R., Bibler, T., Childress, A. M., Stephens, A. L., Pena, A. M., & Allen, N. G. (2016). Navigating Ethical Conflicts Between Advance Directives and Surrogate Decision-Makers’ Interpretations of Patient Wishes. Chest,149(2), 562-567. doi:10.1378/chest.15-2209
1 Comment
|

Alexander McNaChronicles of my journey into the nursing profession. Archives
September 2018
Categories |
 RSS Feed
RSS Feed
